Decalcification of the Pineal Gland
A grain-of-rice gland makes the most powerful psychedelic known, runs your master clock, and most adults are turning it to stone. The chemistry that reverses it.
A grain-of-rice organ at the geometric centre of your brain manufactures the most powerful psychedelic compound known to man, and right now it is turning to stone.
The same gland runs the body's master clock, builds the architecture of sleep, and seeds the chemistry that long-term meditators arrive at after decades of practice. Most adults are calcifying it, and age is not the cause. The deposits start in childhood and track the load the body carries: fluoride, bromide, heavy metals, arriving faster than they are cleared. Age looks like the cause only because it gives the load more time.
The decline is gradual. Sleep flattens. Dreams lose their lawful physics. Mornings stop arriving clean. The sense of being "in tune" that most people remember from their twenties and cannot quite locate in their forties is not a memory of youth, it is a memory of an uncalcified gland doing its job. The condition feels like normal aging. It is not. The calcification is reversible, and the chemistry that reverses it is well characterised.
The pineal does not produce a chemical that delivers experience. It produces a chemical that builds the architecture experience runs on.
What you get back
Restored pineal function returns a specific list, each item mapped in the literature, none of it folklore.
- Sleep architecture. Melatonin output rises, the night-time peak sharpens, slow-wave and REM cycles deepen. The first hour of the morning lands clean instead of foggy.
- Dreams with lawful physics. Vivid, continuous, navigable. The substrate the older traditions called the dream body returns.
- Lucid dreaming becomes accessible. Meta-awareness inside the dream depends on intact REM and pineal tryptamine output. Training works only to the extent the chemistry is in place.
- Tighter phase relationships. Morning cortisol and night melatonin lock back into their inverse partnership. The whole hormonal cascade, thyroid, adrenal, gonadal, drifts back on rhythm.
- Meditative depth. The gamma-band synchrony and quieted default-mode that long-term meditators reach by discipline becomes reachable in fewer sittings.
- The "in tune" sense. A baseline coherence, a felt alignment between the inner clock and the world outside, returns within four to six weeks of consistent adherence.
The reward is the use of a faculty most adults spend their middle decades without realising they have lost.
The biology, what the gland actually does
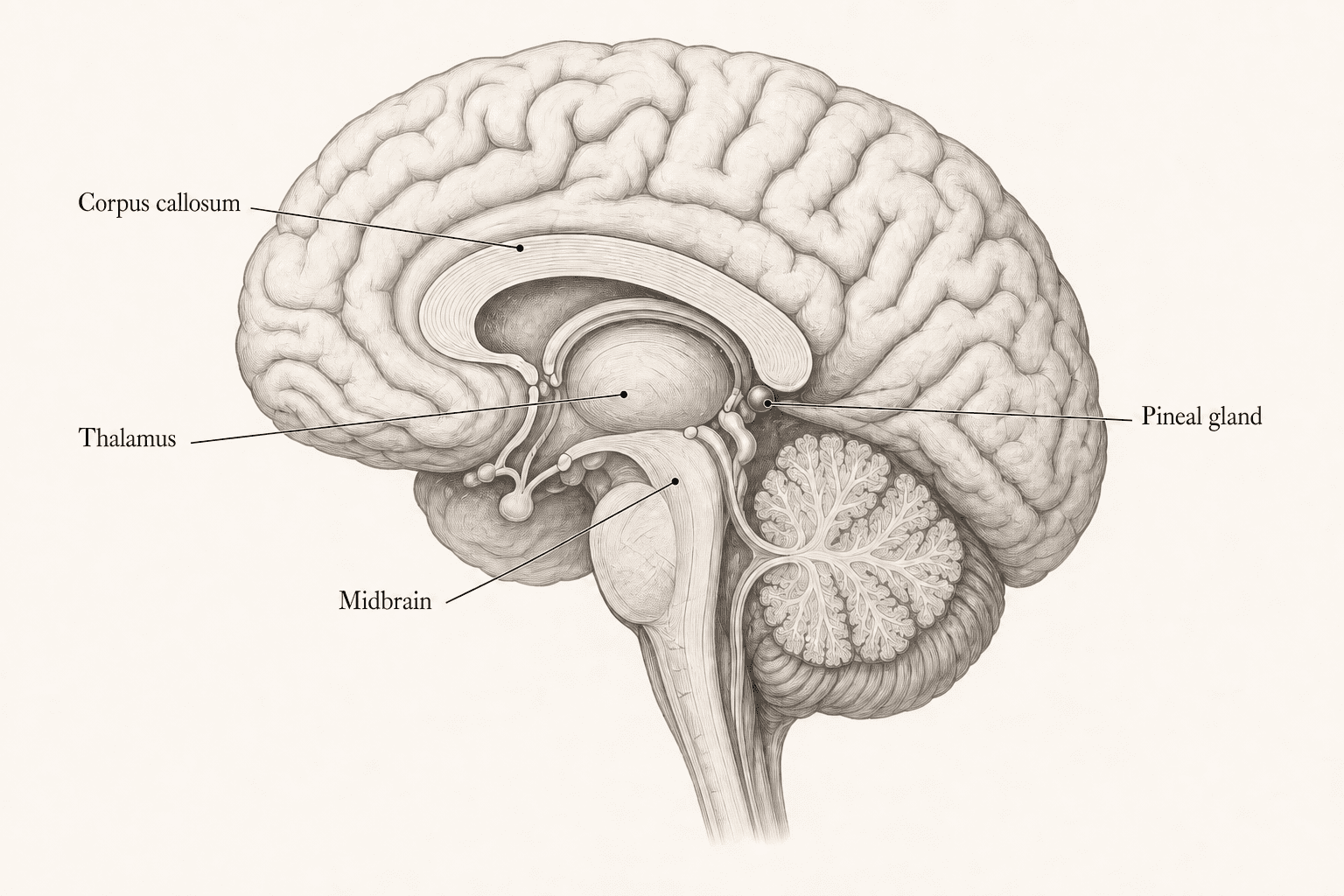
The pineal is the smallest hormone-making organ in the body, and one of the most consequential. It is the size of a grain of rice. It sits at the geometric centre of the brain, in a small chamber called the , just above a small pool of cerebrospinal fluidfootnoteAnatomically the gland is unique, it lies outside the blood-brain barrier, drawing its blood supply directly from branches of the posterior cerebral arteries. That privileged position is what makes it both metabolically rich and uncommonly vulnerable to substances circulating in the blood, including the calcifying agents that accumulate in it through life.. For its size it receives more blood than any organ in the body other than the kidney.
Its main job is to make , the hormone that runs the body's clock. Without it the architecture of sleep collapses, the immune system loses some of its night-shift surveillance, and the whole hormonal cascade drifts off rhythm.
The pineal does more than release melatonin at dusk. It makes a small family of related molecules that modulate the brain's main neurotransmitters, dopamine, serotonin, GABA, glutamate. It shapes mood, cognitive flexibility, and the texture of dreaming. When it works, sleep is restorative, mornings are clean, and the daily rhythm of the nervous system tracks the sun. When it doesn't, none of those things do.
The other molecule the gland makes, DMT
Set melatonin to one side. The pineal also makes , the same molecule the body produces in trace amounts under specific physiological conditions. The pathway is well characterised: the amino acid tryptophan is converted to tryptamine, then to DMT, by footnoteBarker, S. A. et al. (2013). Drug Test Anal. INMT expression has been mapped in pineal, retina, lung, and spinal cord tissue in mammals. The 2013 Barker and Borjigin analytical paper confirmed measurable N,N-DMT in living-rat pineal microdialysate at concentrations comparable to serotonin..
In 2013, Barker and Borjigin measured DMT in the pineal of living rats at concentrations comparable to serotonin.
Psilocybin takes hold over an hour. LSD runs most of a day. DMT is dosed in milligrams by smoked weight and produces, in the dose window, a complete dissolution of ordinary perception inside thirty seconds, peaking at three minutes, fully metabolised inside fifteen.
Nothing else in the psychopharmacology of consciousness comes close to that speed and completeness, and nothing else is endogenous. The pineal is the only organ on the inventoried list of mammalian tissue that produces DMT and sits at the geometric centre of the brain.
What DMT does to the brain
When DMT reaches the brain it docks onto , the same one most psychedelics use, with smaller effects on a couple of others. Three measurable things happen.
First, the brain literally grows new connections. The same receptor activation that produces the subjective shift triggers , a growth response in the neurons themselves: new branches, new connection points, a denser web of wiring. The Olson lab at UC Davis showed in 2018 that a single dose at physiologically relevant levels produced changes that persisted for weeks.
Second, the brain's frequencies synchronise. Brainwave recordings during deep contemplative states, measured most cleanly in long-term meditators, show firing in lockstep across the frontal and parietal cortex. Lutz and Davidson's work with Tibetan monks at Madison found this synchrony at thirty standard deviations above novice baseline. That is what practitioners describe as a unitary or non-dual state: the brain's binding clock running at a tempo that integrates experience rather than fragmenting it.
Third, the inner critic goes quiet. The , the rumination machinery, the inner narrator, drops in activity. What remains is the underlying perceptual field, less filtered, more bare. fMRI studies of advanced meditators show the same signature in deep states. So do studies of sub-perceptual psilocybin microdoses.
The dream-state correlation
The clearest in-body evidence for endogenous DMT activity is REM sleep.
Melatonin output peaks in the same window as the deepest dreaming phases, between 02:00 and 04:00 local time, and the brain-wave pattern of REM looks, in topology, very similar to the pattern seen under controlled administration of DMT from outside the body. Strassman's original hypothesis, the one that gave his book The Spirit Molecule its title, was that the gland's own DMT release at the threshold of deep REM is what generates the hyperreal phenomenology of dreaming. The mechanism fits the chemistry. The overlap is unmistakable: vivid sensory environments, narrative continuity, lawful dream-physics, the precise signature of a tryptamine state generated from inside the skull.
This is why lucid dreaming and the pineal are tied together in a way most popular treatments miss. The capacity to recognise a dream as a dream while inside it depends on:
- Enough melatonin to support deep REM cycles
- Enough cortical activation to keep meta-awareness alive during the dream, modulated by the gland's tryptamine release
- Enough pre-sleep priming of the prefrontal "is this a dream?" check, a training effect, not a chemistry effect
The first two depend on what the gland is putting out. A calcified pineal underdelivers both. The third, the training, only works to the extent the first two are intact. Lucid dreaming becomes vastly more accessible once sleep architecture itself is restored, which is exactly what decalcification supports downstream.
Meditation and the consciousness loop
Long-term meditation reaches the same neural endpoint by a different route. Sustained attention practices, Vipassana, Zen shikantaza, Tibetan rigpa, produce the same fast synchronised rhythm, the same quieting of the inner narrator, and, over decades of practice, measurable thickening of the cortex and tighter in the same regions that DMT activates acutely. A chemical lever and a discipline lever, both arriving at the same place.
The bridge is that sustained attention itself triggers small endogenous DMT release at the pineal, which is why advanced practitioners describe states phenomenologically indistinguishable from exogenous DMT experiences without having taken anything. The gland is doing the work; the practice gives it the cue.
This is the case for treating pineal function as a substrate, not just a circadian regulator. The gland is not separate from the work of the mind.
It is one of the organs by which the mind builds itself.
What calcifies it
The deposits visible on CT and MRI, detectable even in children and thickening with every year of toxic exposure, are , the same calcium-phosphate crystal the body uses to make bone, accumulating in the pineal because the gland's high blood flow, lack of blood-brain barrier, and capacity to concentrate certain ions make it a sink for substances the body is trying to sequester.
The gland is not failing. It is being used as a dumping ground.
Three classes of input accelerate the process.
- Fluoride, bromide and chlorine crowd iodine out. They are all , chemical cousins that share the same docking points in the body, and when iodine is in short supply they take its place. Fluoride is the worst of them, it concentrates in this little gland more than in any other soft tissue in the body. In 1997 the researcher Jennifer Luke measured fluoride levels inside calcified pineal tissue at 21,000 parts per million, higher than in bones already damaged by chronic fluoride exposure. Halide saturation is, in part, an iodine-deficiency disease.
- Heavy metals get caught in the calcium current. Aluminium, lead and mercury accumulate in any tissue that is busy mineralising. The pineal's affinity for calcium drags them along.
- Chronic low-grade inflammation and low magnesium. Magnesium is the body's main brake on the wrong kind of calcification. When magnesium is low, calcium deposits readily in soft tissue, arteries, joints, glands. Add silent inflammation, and the substrate for calcification is laid down faster than the body can clear it.
The consequence arrives slowly. Melatonin output falls in step with the calcified fraction, and every rhythm downstream of it loosens by the same degree. Nobody notices the year it starts. They notice the decade it has been running.
The protocol
It is built around three principles: displace the halides (give the body the iodine it actually needs so fluoride and bromide leave the receptor sites), supply the cofactors of decalcification (the minerals and vitamins that route calcium back into bone and away from soft tissue), and support the exits (the liver, the bile, and the bowel, the roads the displaced load leaves by).
Seven items, each pinned to a specific layer of the problem.
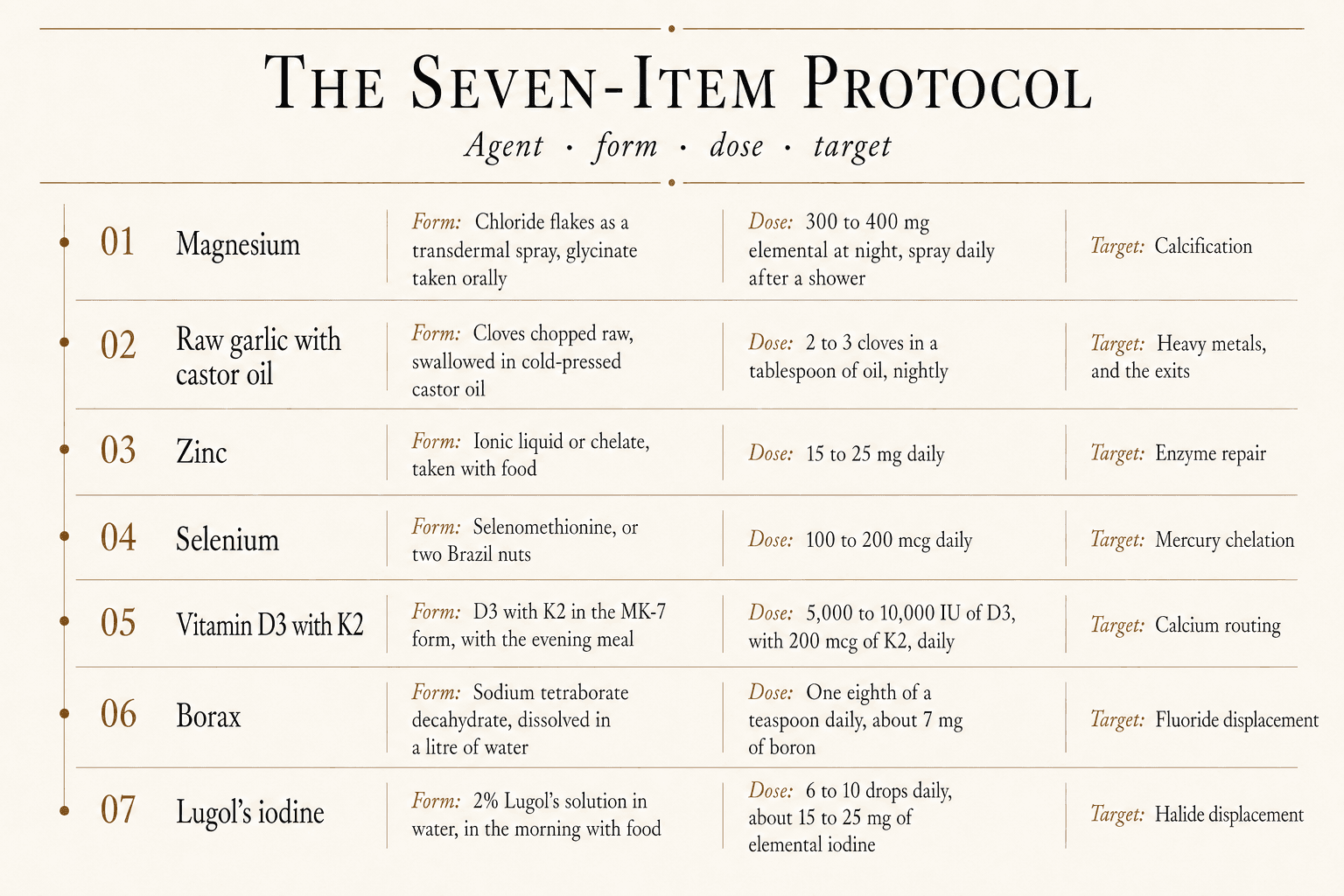
1. Transdermal magnesium chloride and oral magnesium glycinate, daily
Two routes, one mineral. The transdermal route is a spray bottle of magnesium chloride flakes dissolved in distilled water, roughly one part flakes to one part water by weight, applied after a shower to the inside of the forearms, the chest, the abdomen and the calves.
Let it sit for 20-30 minutes, then rinse off the white residue.
Alongside the skin route, 300-400 mg of elemental magnesium taken orally at night as . Glycinate is one of the two strong oral forms, alongside the magnesium bicarbonate water in the minerals essay, because it bypasses the limitation that has historically made oral magnesium useless at the doses that actually move tissue levels.
Magnesium citrate, oxide and sulphate trigger an osmotic effect in the gut, drawing water in and producing loose stools long before serum or tissue magnesium rises meaningfully. Glycinate is bound to the amino acid glycine, which carries it across the gut wall on the amino-acid transporter system, and the glycine itself is a calming neurotransmitter that supports the same deep-sleep architecture the rest of the protocol is aimed at restoring.
Magnesium is the most under-supplied mineral in the modern diet and the central counter-force to pathological calcification. It is required for over 300 enzymatic reactions, including every step of how the body uses ATP, the cell's energy currency. It is the cofactor for converting vitamin D into its , for binding calcium into bone (instead of soft tissue), and for the body's manufacture of .
The two routes are complementary. Transdermal delivers magnesium ions directly into the dermal microcirculation, useful for loading volume without going through the gut. Oral glycinate adds a steady intracellular dose with a calming side-benefit and is the more practical lever for anyone who travels or wants a single capsule instead of a spray ritual.
For the pineal specifically: magnesium is what pulls calcium out of soft tissue and routes it toward bone where it belongs.
2. Raw garlic, chopped, with castor oil, at night
Two to three cloves of raw garlic, chopped finely, swallowed in a tablespoon of cold-pressed castor oil before bed.
The active compound in garlic is , a sulphur compound formed when the clove is crushed. It is one of the most potent natural we know offootnoteCha, C. W. (1987). Tohoku J Exp Med. Allicin chelates heavy metals including lead, mercury, and cadmium. The protective effect against acute heavy-metal toxicity in animal models is large and consistent..
It grabs onto lead, mercury and cadmium, and routes them through the liver for excretion. It is also broadly antimicrobial against the gut bugs that drive chronic systemic inflammation, including some of the organisms implicated in what's increasingly called the gut-pineal axis, the subject of the parasite cleanse essay.
The castor oil is the mechanical half. Its keeps the bowel moving and stimulates the flow of bile, so the metals the garlic has bound leave overnight instead of cycling back through the , and the parasite cleanse essay sets out the full pharmacology. Because the same receptor contracts the uterus, castor oil is contraindicated in pregnancy.
3. Zinc, ionic or chelated
15-25 mg of zinc, as an ionic liquid or a chelate, taken with food, daily.
Zinc is the second most abundant trace mineral in the body and one of the most under-supplied. It is the cofactor for over 300 enzymes, including the , the main pathway the body uses to lock up and remove heavy metals.
Without enough zinc, that system runs at half speed, and copper, cadmium and mercury accumulate instead of leaving.
Specific to the pineal: zinc is required for the body to convert serotonin into the chemical that becomes melatonin. Low zinc means low melatonin no matter what else is in place.
Form matters. An ionic zinc solution sits at the top of the absorption ladder, and a chelate, picolinate, citrate or bisglycinate, is the strong second. Much commercial zinc is the oxide form, which the gut barely absorbs and largely passes straight through. Mineral form, ionic against chelated against cheap inorganic salt, is the whole subject of the supplement essay.
4. Selenium
100-200 mcg of selenium daily, ideally as selenomethionine, or as two Brazil nuts.
Selenium is the cofactor at the heart of two critical systems. The first is , the enzyme that keeps the body's master detox molecule recyclable. Without selenium, that system runs into deficit and the body's capacity to remove fat-soluble toxins and heavy metals collapses.
The second is the family of that convert storage thyroid hormone into its active form. A selenium deficiency produces a quiet kind of low thyroid that doesn't show up on standard TSH tests but produces every clinical symptom of it, and a sluggish thyroid throttles the pineal downstream.
For pineal-specific work, selenium is also one of the few minerals that directly binds mercury, forming inert complexes the kidneys can excrete. Mercury exposure is one of the underweighted drivers of soft-tissue calcification.
5. Vitamin D3 with K2
5,000-10,000 IU of vitamin D3 daily, paired with 200 mcg of vitamin K2 in the MK-7 form.
Vitamin D3 is a hormone, not really a vitamin. It regulates the expression of more than 2,000 genes and tells the gut how much calcium to absorb.
K2 is the cofactor for that decide where the absorbed calcium ends up: one routes it into bone, the other actively keeps it out of arteries and soft tissue.
This is the calcium paradox, and the pineal is why it belongs here as well as in the minerals protocol. D3 decides how much calcium the gut takes up. K2 decides where it lands. Without K2, a share of it lands in glandular tissue, and this gland is glandular tissue at the exact centre of the head. Take them together with the evening meal, alongside the magnesium D3 needs for its activation step.
6. Borax, one-eighth teaspoon daily
A small amount of , sodium tetraborate decahydrate, dissolved in a litre of water and sipped through the day.
Borax is the dietary source of , a trace mineral that the industrial diet has largely lostfootnoteDevirian, T. A.; Volpe, S. L. (2003). Crit Rev Food Sci Nutr. The boron content of food has declined with industrial agriculture; supplementation at 3-10 mg/day shows benefits across multiple endpoints from bone density to cognitive performance..
Boron supports cell membrane integrity, regulates inflammation, and helps vitamin D and magnesium do their jobs. Critically here: it directly competes with fluoride for the sites where fluoride would otherwise accumulate, displacing it from bone and soft tissue.
One-eighth of a teaspoon of borax in a litre of water yields about 7 mg of boron, inside the range that has shown anti-inflammatory and bone-density benefits in controlled trials. The salt also delivers a small alkalinising load that helps the kidneys excrete the freed fluoride.
A point of precision: there is only one borax, the same mineral whether the label sells it as a cleaner or as a supplement. What changes is the dose, and an eighth of a teaspoon is the dietary one. Hold it there, and stop if you notice any irritation.
7. Lugol's iodine, 6 to 10 drops daily
Six to ten drops of in water, taken in the morning with food.
Iodine is the master halide. When iodine is present in sufficient amount, the body's halide docking sites are occupied with iodine, and the other halides, fluoride, bromide, chlorine, are excreted instead of accumulating. When iodine is deficient, the docking sites are filled by the others, with consequences for the thyroid, breast, prostate and pineal.
Those drops deliver roughly 15-25 mg of elemental iodine, substantially above the standard daily recommendation, which is set at the minimum required to prevent goitre and is widely considered insufficient for full-system iodine sufficiencyfootnoteThe RDA of 150 mcg/day was established to prevent overt goitre and cretinism. Optimal iodine status, measured by 24-hour urinary iodine after a loading test, runs in the 12-25 mg/day range per the work of Abraham, Brownstein, and Flechas. The IodineProject literature is the canonical reference for the high-dose iodine protocol..
The Japanese coastal diet provides 12-25 mg/day from kelp, and the public-health record of those populations on hormone-sensitive cancers and thyroid disease is strikingly favourable.
For the pineal specifically: iodine sufficiency is what allows the gland to eject the fluoride it has accumulated. Decalcification without iodine is grinding against a clutch that is still engaged. Iodine releases it.
Cofactors matter. Iodine loads more efficiently in the presence of sufficient selenium, which buffers the that iodine triggers as halides are displaced, and magnesium, which supports the whole detoxification cascade. The protocol is designed around this. Iodine is the lever; the other items are the fulcrum.
The arc
Decalcification is not a one-week project. The literature on heavy-metal mobilisation suggests three to nine months for visible reduction on imaging, and then lifelong maintenance.
The subjective changes, depth of sleep, vividness of dreams, clarity in the first hour of the day, show up earlier, usually within four to six weeks of consistent adherence. The discipline is the protocol. The reward is the gland that was built to keep time, keeping it again.
Clearing the gland is only half the circuit. A pineal freed of its stone is a receiver brought back online, and the signal it was built to track comes from outside the skull: the daylight that sets the clock through the eye, and above all the low sun of morning and evening. The current runs outward from here, to the electric body and the practice of taking light from the sun.
Sources
- The pineal gland and melatonin in relation to aging, . https://pubmed.ncbi.nlm.nih.gov/7715064/
- Calcification of the pineal gland in childhood,
- Fluoride deposition in the aged human pineal gland, . https://pubmed.ncbi.nlm.nih.gov/11275672/
- Magnesium in man, implications for health and disease,
- Vitamin K2 and the calcium paradox,
- Iodine deficiency in industrialized countries,
- N,N-Dimethyltryptamine and the pineal gland, separating fact from myth, . https://pubmed.ncbi.nlm.nih.gov/22841895/
- Psychedelics promote structural and functional neural plasticity, . https://pubmed.ncbi.nlm.nih.gov/29898390/
- Long-term meditators self-induce high-amplitude gamma synchrony during mental practice, . https://www.pnas.org/doi/10.1073/pnas.0407401101
- DMT, The Spirit Molecule,
Next in the series
The Incorruptible Body · The LightSungazing and the Electric BodyYou are a column of salt water conducting between a fusion reactor and a charged planet, and modern life unplugged you at both ends. How to drink light safely, the hand poses that widen the dose, why bare earth recharges the system, and the honest truth about living on light.
- Published
- Reading
- 13 min
- Sources
- 10