Lemon and Bicarbonate
The five-cent morning drink that hands the body back its acid-base buffer, and the chemistry of why it works.
Right now, between the words you are reading, your body is quietly robbing your own skeleton. Every minute you spend without enough bicarbonate, it dissolves calcium and magnesium out of your bones to neutralise the acid that ordinary living produces, because the alternative is letting your blood pH drift outside the band that keeps your enzymes alive. The juice of one whole lemon and a teaspoon of in twelve ounces of water, taken first thing in the morning, stop the theft. They hand the body back the buffer it has been borrowing from your bones, and they push the first-void urinary pH into the window where the kidneys actually start excreting the day's metabolic acid load. The clinical literature on alkaline buffering is good. The protocol is older than pharmacology. The total cost is under a dollar a day.
Most chronic disease runs in a body that has been spending its buffer faster than it replaces it. The drink fixes that at the source. Its effect on baseline energy, sleep depth, digestion, and the daily detoxification work the liver and kidneys do is out of all proportion to the price.
If there is one thing you could do every day that would dramatically fight disease and increase your energy, consuming lemon juice combined with baking soda would be on the top of the list.
That is Dr. Loyd Jenkins of the Budwig Center. He is right, and what follows is the chemistry of why.
What you get back
Seven things. The chemistry behind each one is worked out below.
- Restored acid-base buffering. A higher keeps you out of the bottom band, where all-cause mortality ran 24% higher in the Raphael 2017 cohort. Most physicians never surface the number.
- More efficient oxygen delivery. The bicarbonate-buffered CO2 reserve is what lets haemoglobin actually let go of oxygen at the tissue that needs it. Same breathing, more oxygen where it counts.
- Deeper sleep. The brain's overnight waste-clearance work runs on adequate tissue oxygenation.
- Cleaner mornings. No "wake-up acid" feeling, and a bowel that moves the way it should.
- Mineral conservation. Supply the buffer directly and the body stops pulling calcium and magnesium out of bone to do the work. Less muscle cramping, less of the calcification cascade traced in the pineal essay.
- A daily dose of citrus bioactives. Around 50 mg of vitamin C and the citrus flavonoids that ride across in the juice.
- Citric acid for free. A few grams a day, with its own cancer-metabolism story.
All of that from the juice of one lemon and a spoonful of baking soda, taken before breakfast.
The biology, why CO2 is the lever
Squeeze a lemon into water, stir in a teaspoon of baking soda, and the solution fizzes, visibly, audibly, for thirty seconds. That is real chemistry, and the same reaction keeps going inside the stomach.
The reaction:
NaHCO3 + HCl yields NaCl + H2O + CO2
In the glass, baking soda plus the lemon's citric acid yields , sparing some of the stomach's own acid for digesting the food that follows.
The carbon dioxide is the point. It is not waste. It is one of the most consequential signalling molecules in human physiology.
The modern understanding of its role began with two researchers at the end of the nineteenth century, Christian Bohr in Denmark and Bronisław Verigo in Russia. Working separately, they discovered the same counter-intuitive law: oxygen does not come off the blood's oxygen carrier without carbon dioxide present.
The is this: , the blood's oxygen carrier, releases its oxygen only where there is enough carbon dioxide in the surrounding tissue. Sprinting muscle, a thinking brain, a wound healing itself, all make the most CO2, which is the body's way of saying deliver oxygen here. Without CO2 in the picture, the oxygen stays locked to the haemoglobin and the tissue starves even though the blood itself is full of oxygen.
This is why during anxiety produces the symptoms it does. The patient blows off CO2 faster than the tissues make it. Haemoglobin clamps down. The brain, the body's most oxygen-hungry organ, feels the shortage first, which feeds the anxiety, which feeds the breathing. A tightening loop, and the way out is the same chemistry: get carbon dioxide back into the system.
Oral baking soda on an empty stomach with lemon raises the body's blood bicarbonate level, and a higher bicarbonate level is, in effect, more carbon dioxide stored in chemically buffered form. The body carries more reserve. Tissue oxygenation runs more efficiently for the same amount of breathing. This is what Dr. Sircus has called CO2 medicine, and almost no one in modern preventive practice is using it.
What blocks it, the acid load most people carry
The body defends blood pH ferociously, between 7.35 and 7.45, the band every enzyme depends on.
Without adequate bicarbonate, the daily acid produced by protein digestion, stress, exercise, and the modern diet would shift the blood outside the survivable range within hours. So the body finds the buffer somewhere. Under-supply bicarbonate and it pulls calcium and magnesium out of bone to do the buffering instead.
Chronic low-grade acidity is one of the inputs to the calcification problem traced in the pineal decalcification protocol and the eight-item mineral stack. Bone mineral leaches out, acid is neutralised, and the now-circulating calcium has to land somewhere.
Without enough magnesium and vitamin K2 to route it, it deposits in arteries, joints, and soft tissue. The lemon-and-bicarbonate drink interrupts that loop at the cheapest possible point.
The longevity correlation
In 2017 Dr. Kalani Raphael's team at the University of Utah published an analysis of in community-dwelling older adults. The finding was direct: low blood bicarbonate carried a 24% higher risk of premature death, independent of every other risk factor they controlled for.
Raphael's commentary: "What we found was that generally healthy older people with low levels of bicarbonate had a higher risk of death."
Standard clinical practice does not measure this routinely; the number sits buried inside the basic metabolic panel and is rarely surfaced as a risk factor. It should be. Bicarbonate sufficiency tracks with mortality the way LDL tracks with cardiovascular events, more cleanly and far more correctable, and the cheapest intervention available to correct it is a teaspoon of food-grade baking soda a day.
The cancer-as-fungus framing
Dr. Tullio Simoncini, the Italian oncologist, has built his career on the finding that , growing in low-oxygen, acidic local environments and responding to high-dose bicarbonate the way a fungal infection responds to an antifungal. He has used intravenous baking soda as a primary cancer intervention, with reported regressions across various tumour types.
The underlying biology is settled. that cancer cells preferentially burn glucose in a wasteful, oxygen-skipping way and acidify the tissue around them is foundational cancer biology. Baking soda raises the local pH and stresses the tumour environment. The high-dose IV is a physician-supervised intervention. The daily oral teaspoon, taken as a preventive, is the floor anyone can run at home.
What the juice actually is
A lemon is not a vitamin C delivery device. The juice of one fruit carries about 50 mg of vitamin C, a reasonable daily share, and it carries the citrus flavonoids, hesperidin and eriocitrin chief among them, each with its own vascular and anti-inflammatory effect.
The juice also delivers , which carries its own metabolic story. Dr. Alberto Halabe Bucay has run a treatment protocol on cancer patients using 10-15 grams of pure citric acid orally three times a day, paired with a stomach-protective drug to spare the stomach lining. His proposed mechanism: citric acid jams the that cancer cells depend on more heavily than normal cells do. He has reported clinical improvement in over 80 cancer patients on this regimen.
Daily lemon hands you a few grams of citric acid as a side effect of everything else the fruit is doing.
The protocol
Every morning, before food, before coffee, before anything else.
The recipe
- The juice of one whole organic lemon, squeezed straight into the glass. Nothing more elaborate than that.
- One teaspoon (~4 g) of food-grade baking soda. Pure, aluminium-free, from a reliable supplier. Some morning rotations include half a teaspoon of as well, to balance the sodium dose.
- 12 ounces of room-temperature distilled water, not cold, not hot. Cold suppresses the reaction; hot flattens the fresh juice.
- Stir, let the visible fizz settle, drink. The fizz is the citric acid and the bicarbonate reacting off as CO2; what stays in the glass is sodium citrate plus the bicarbonate that did not react, and the body converts the citrate back into bicarbonate downstream. Either way the alkaline buffer lands.
When and why
Morning, on an empty stomach. This is the highest-leverage window. Overnight the body has been running on its bicarbonate reserves and has accumulated an acid load from ordinary cellular work; the morning dose resets the buffer and delivers the vitamin C and citric acid when absorption is at its peak.
A second dose 30 to 45 minutes before bed, on an empty stomach away from food, supports the overnight detoxification and the deeper sleep phases, the dose that most affects subjective sleep quality. The carbon-dioxide effect of the baking soda is most useful for the brain, which spends the night doing , and the mineral-conservation effects support that process.
Avoid taking it with meals.
The baking soda neutralises stomach acid, and you want stomach acid for the protein digestion that comes with food. Stay 60+ minutes away from any meal.
The hard limit on the protocol is sodium.
A teaspoon of baking soda is roughly 1.2 g of sodium, within the daily allowance but cumulative if you are already eating a high-sodium diet. People with hypertension or kidney disease should consult a physician and probably substitute the potassium form for the sodium form.
The other side of the balance, apple cider vinegar
Everything above is one half of a two-sided system, and it is the half most people are short of. It does not follow that more alkalinity is always better. The body is not trying to be alkaline, it is trying to regulate, and regulation needs both hands: an alkaline reserve to neutralise the acid of ordinary metabolism, and enough acid to digest protein, free minerals from food, and dissolve what has hardened where it should not be. Take either side away and the regulator loses its grip. That is the mistake buried in the alkaline-water business, which sells the idea that a body pushed further alkaline is a body doing better. It is worth naming here so the morning drink is not read as a push in one direction. Bicarbonate refills the reserve. It does not drive the body alkaline, and it should not.
The acid side has its own daily instrument, and it is raw apple cider vinegar.
A tablespoon in a glass of water is one of the most useful things in the kitchen. It carries acetic acid, which sharpens digestion and blunts the glucose rise that follows a meal, and it carries malic acid, the same acid that softens hardened cholesterol through the six days of preparation before a liver flush. What malic acid does to a gallstone it does more slowly to the calcium the body has parked where it does not belong. Acid mobilises mineral. A body with enough of it keeps its calcium in solution and moving; a body running short parks it in arteries, joints, and soft tissue, which is the same cascade the bicarbonate works against from the other end. The two are hands on the same problem.
Keep them apart in time. Vinegar and bicarbonate in one glass cancel each other on contact, spend themselves as fizz, and deliver neither. Take the lemon and bicarbonate on an empty stomach as above. Take the vinegar before a meal, where the acid has work to do, and leave at least an hour between them.
The sourcing is not a footnote. Apples carry one of the heaviest pesticide loads of any commercial crop, and vinegar is a concentrate: what was on the fruit ends up in the bottle, sharpened rather than diluted. Non-organic apple cider vinegar, and anything fermented carelessly, delivers a concentrated dose of whatever was sprayed on the orchard, which is the exact opposite of what you are drinking it for. Buy it organic, raw and unfiltered, with still in it, and in glass, because the acid pulls plasticiser out of a plastic bottle over the months it stands in a cupboard.
The arc, what to expect
- Within the first week: deeper sleep, clearer mornings, less of the classic "wake-up acid" feeling. Bowel motility usually improves within the first three days.
- Within the first month: clearer skin from the fibre plus the vitamin C, less muscle cramping from the bicarbonate-conserved magnesium, steadier energy across the day.
- Beyond three months: the trend lines on blood bicarbonate (if your physician will pull it) and on first-morning urine pH (which you can test daily with strips for a few dollars) move into the upper end of the normal range. That is the measurable proof, and it is the one to track.
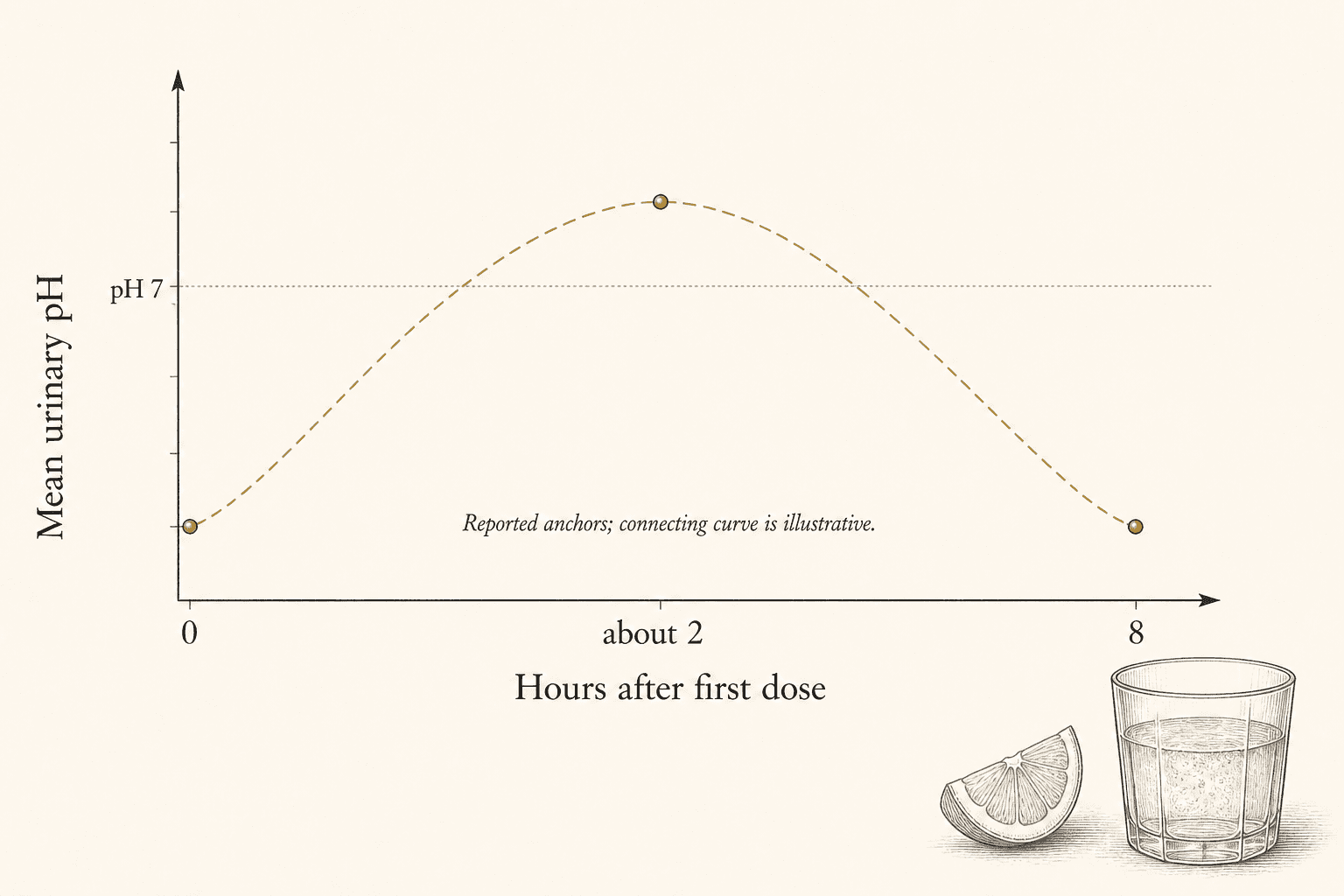
Cohen and colleagues put numbers on the curve. Nine healthy men took 4 g of oral sodium bicarbonate at time zero. Mean urinary pH was above 7 at about two hours and back to baseline by eight, which is exactly why the dose repeats through the day rather than carrying it alone.footnoteCohen, B. et al. (2013). "Efficacy of urine alkalinization by oral administration of sodium bicarbonate: a prospective open-label trial." American Journal of Emergency Medicine 31(12):1703-1706. Nine healthy men received 4 g at 0, 8, and 16 hours. Baseline at dosing, mean pH above 7 at about 2 hours, return to baseline by 8 hours. DOI: 10.1016/j.ajem.2013.08.031.
The wider context
This protocol does not stand alone. It is the cheapest, most accessible foundation of a wider mineral and acid-base practice that includes the eight-item mineral stack, the seven-item pineal decalcification protocol, adequate hydration, daily sun exposure, and the slow-breathing practice that drives up and pushes the same Bohr-Verigo physiology forward by a different lever.
The cheapest medicine in the house is the one the body recognises fastest.
But the buffer can only neutralise the acid that arrives. The largest single source of that daily acid load is the food on the plate, and here the conventional wisdom has it exactly backwards.
The diet sold as the clean, light, virtuous one, the one that promises to alkalise and heal, is quietly starving the body of the very minerals and proteins it needs to build its own buffer and its own structure. That is the next thing to take apart.
Sources
- Inhibition of cancer cell growth by citric acid (Bucay protocol),
- Serum bicarbonate and risk of mortality in community-dwelling older adults, . https://pubmed.ncbi.nlm.nih.gov/28298322/
- Efficacy of urine alkalinization by oral administration of sodium bicarbonate, . https://pubmed.ncbi.nlm.nih.gov/24055481/
- The Bohr-Verigo effect, CO2's role in haemoglobin oxygen release,
- Sodium Bicarbonate (Second Edition),
Next in the series
The Incorruptible Body · The GroundSoil Death and the Case for Animal Foods, Why Most Plant-Based Diets Fail in a Depleted CenturyIndustrial soil no longer holds the elements every cell needs, so the plant inherits the deficiency and the animal is the only thing that concentrates it back. The genetics that decide who can run a plant diet, and the exact discipline a vegetarian must run not to break underneath it.
- Published
- Reading
- 9 min
- Sources
- 5